Aneel Bhangu, Surgical Data Institute, Department of Applied Health Sciences, University of Birmingham, Birmingham, UK
DOI: 10.5281/zenodo.20592763
The wound closure literature is, by any reasonable measure, deeply unsatisfying. Multiple randomised controlled trials have evaluated antiseptic irrigation, suture material, incise drapes, antimicrobial dressings, and topical agents, with many recording no statistically significant effect on the primary endpoint. Even taking into account those that do, the dial on population wound infection rates has not shifted far, despite the financial investment into research. The reflex interpretation is that the interventions do not work and money should be wasted, but a more accurate interpretation is that the trials require a firm re-design and the marginal gains of interventions should not be ignored.
Surgical site infection (SSI) defined by Centers for Disease Control and Prevention criteria¹ is the incumbent standard. It is internationally recognised, operationally simple, and amenable to post-discharge telephone surveillance.¹ Its limitation from the standpoint of trial design is that a binary infection (yes or no) captures only one component of the wound morbidity spectrum. Dehiscence, seroma, and haematoma each contribute meaningfully to delayed recovery and resource use and are left out of SSI trials. Such SSI definitions were designed for institutional surveillance programmes, not for evaluating marginal gains in complex interventional strategies.
There are alternatives including the ASEPSIS scoring method and Southampton wound grading scale that capture dehiscence, seroma, and haematoma alongside infective features.²·³ What they do not readily resolve is the primary endpoint problem. Ordinal systems require a binary event, still creating problems with sample size requirements.
In the minimally invasive era, with baseline SSI rates falling as laparoscopic and robotic approaches become standard, the absolute effect attributable to any single closure component is modest. A 20% relative reduction in SSI from a 15% baseline represents an optimistic estimate for any single intervention. To detect that effect using binary SSI at 90% power requires 2,723 patients per arm, 5,446 in total, with the high risk of a negative outcome.
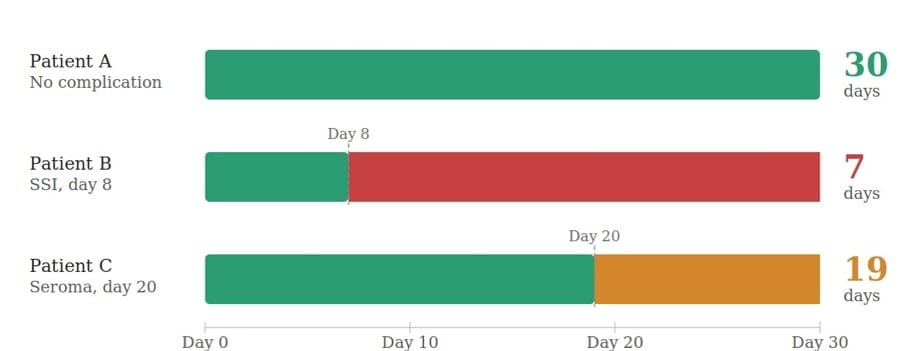
Days Alive Without Wound Complication at 30 days (DAWC30) offers a tangible solution. Modelled on the ventilator-free days construct which is standard in acute respiratory distress syndrome trials,⁵ DAWC30 is the number of days from surgery to the first wound complication, encompassing SSI, seroma, haematoma, and dehiscence, capped at 30 for patients completing the period without any wound event. A patient with no complication scores 30; one with SSI on day eight scores seven; one with seroma requiring aspiration on day 20 scores 19. The score is continuous, every patient contributes a value, and it requires only a single structured 30-day notes review and/or telephone assessment.
DAWC30 in an enriched elective gastrointestinal surgery population is heavily right-skewed, with most patients scoring 30 and the remainder clustering near the lower end, reflecting a mean complication onset around day eight. The critical efficiency gains, however, arise from counting all wound complications rather than SSI alone and a continuous outcome. In an enriched population with a 20% all-complication baseline, a bundle producing a two-day improvement in mean DAWC30 score requires 337 patients per arm, 674 in total, at 90% power, using a standard continuous outcome comparison with a pooled standard deviation of eight days. Against 5,446 patients for binary SSI in the same clinical context, that difference is the distance between a trial that can be completed and one that cannot, and a significantly lower research cost.
The second solution of the design challenge is that rather than testing single interventions, wound closure bundles that combine interventions and their marginal gains across multiple operative steps are more likely to show a benefit. These would include combining skin preparation, wound protectors, closure technique, suture types, wound irrigation, and active dressings to reduce complication risk through additive mechanisms.⁴
CDC criteria, ASEPSIS, and Southampton grading each serve legitimate roles as secondary descriptive endpoints and should be used consistently to build the comparative evidence base the field currently lacks.⁶·⁷ The primary endpoint of future wound closure trials should be DAWC30. Until that alignment is achieved, the wound closure literature risks continuing to accumulate trials that were designed, from the outset, not to succeed.
Conflict of interest statement: None declared.
Corresponding author: Professor Aneel Bhangu, Director, Surgical Data Institute, University of Birmingham, UK. a.a.bhangu@bham.ac.uk
References
- Centers for Disease Control and Prevention. Surgical Site Infection (SSI) Event. National Healthcare Safety Network Patient Safety Component Manual. Atlanta: CDC; 2024.
- Wilson AP, Treasure T, Sturridge MF, Grüneberg RN. A scoring method (ASEPSIS) for postoperative wound infections for use in clinical trials of antibiotic prophylaxis. Lancet 1986;1:311–3.
- Bailey IS, Karran SE, Toyn K, et al. Community surveillance of complications after hernia surgery. BMJ 1992;304:469–71.
- Mc Geehan G, Edelduok IM, Bucholc M, et al. Systematic review and meta-analysis of wound bundles in emergency midline laparotomy. Life (Basel) 2021;11:138.
- Meade MO, Cook DJ, Guyatt GH, et al. Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA 2008;299:637–45.
- Wilson AP, Weavill C, Burridge J, Kelsey MC. The use of the wound scoring method 'ASEPSIS' in postoperative wound surveillance. J Hosp Infect 1990;16:297–309.
- Jerath A, Austin PC, Wijeysundera DN. Days alive and out of hospital: validation of a patient-centred outcome for perioperative medicine. Anesthesiology 2019;131:84–93.