
Aneel Bhangu, Surgical Data Institute, Department of Applied Health Sciences, University of Birmingham, Birmingham, UK
DOI: 10.5281/zenodo.20489982
Robotic surgery may never satisfy a conventional incremental cost-effectiveness ratio threshold. Health systems that use this as their primary criteria for adoption are applying a framework designed for a different class of intervention to a platform technology whose benefits are multidimensional and in several respects without precedent in surgery. The more productive questions are what is the most cost-effective configuration of a robotic programme, what clinical outcomes and quality-of-life data are needed to move the cost-effectiveness needle, and what broader dimensions of value should inform adoption decisions while that evidence matures? Cheaper platforms from emerging manufacturers and lap-robotic hybrids will compress capital and consumable costs over time, improving the economics of robotic surgery, but they will not resolve the underlying evaluation problem, because a technology whose full value lies partly outside the cost-effectiveness framework will remain systematically undervalued by that framework regardless of what happens to its price.
The absence of robust quality-adjusted life year data for robotic surgery is not a temporary gap that the next generation of randomised trials will soon fill. QALY calculations require condition-specific, time-limited outcome measurement against a defined comparator, and robotic surgery resists this at almost every level. It spans multiple specialties, indications, and patient populations and its effects on quality of life accumulate across a programme rather than within a single procedure. Many of its most consequential benefits are system-level effects that individual patient-level outcome instruments were not designed to detect. The current cost-effectiveness literature is characterised by wide uncertainty intervals that reflect this absence of adequate data rather than any measured distribution of effect, and health systems should not interpret this uncertainty as evidence.
Clinical outcome data, while still maturing, are directionally encouraging across colorectal, urological, gynaecological, and thoracic surgery. The CLASICC trial established long-term oncological equivalence for minimally invasive colorectal resection1, and Yaxley and colleagues, in the first randomised controlled trial of robotic versus open radical prostatectomy, demonstrated comparable early functional outcomes between approaches in a high-volume setting2,3. Reductions in blood loss, length of hospital stay, and conversion to open surgery have been demonstrated across multiple meta-analyses, though effect sizes remain heterogeneous and long-term oncological equivalence data are incomplete for several indications. These signals define part of the outcome agenda that future health economic analyses will need to address if cost-effectiveness is ever to be calculated with confidence.
The training and digital feedback dimension represents the most genuinely novel value proposition of the robotic platform and the one most invisible to conventional health economic assessment. The surgical black box, encompassing intraoperative data capture, motion analysis, and objective performance metrics derived from the operative environment, creates a continuous record of technical and non-technical performance with no analogue in open or laparoscopic surgery. Jung and colleagues, in the first-year analysis of the OR Black Box study, demonstrated that intraoperative errors and system threats occur at a frequency that retrospective case review cannot capture4, and that the data infrastructure to identify and address these events has transformative implications for surgical training, credentialling, and governance. The robotic platform extends this principle further by generating structured intraoperative data as a native function of the system itself, creating a governance and quality assurance asset whose value extends across the life of a programme and across every trainee who passes through it.
The market trajectory of robotic surgery deserves honest consideration in any value analysis, as robotic pleurality is likely to become common. Chinese manufacturers and lap-robotic hybrid platforms are entering markets at substantially lower price points, and as Sheetz and colleagues documented in their analysis of adoption trends across 73 US hospitals, cost-effectiveness ratios that appear unfavourable at early adoption improve substantially as volume increases and unit costs fall5. This trajectory matters and should inform programme planning, particularly decisions about platform selection and the configuration of multi-robot programmes. It will not, however, close the evaluative gap, because the problem is not solely one of price.
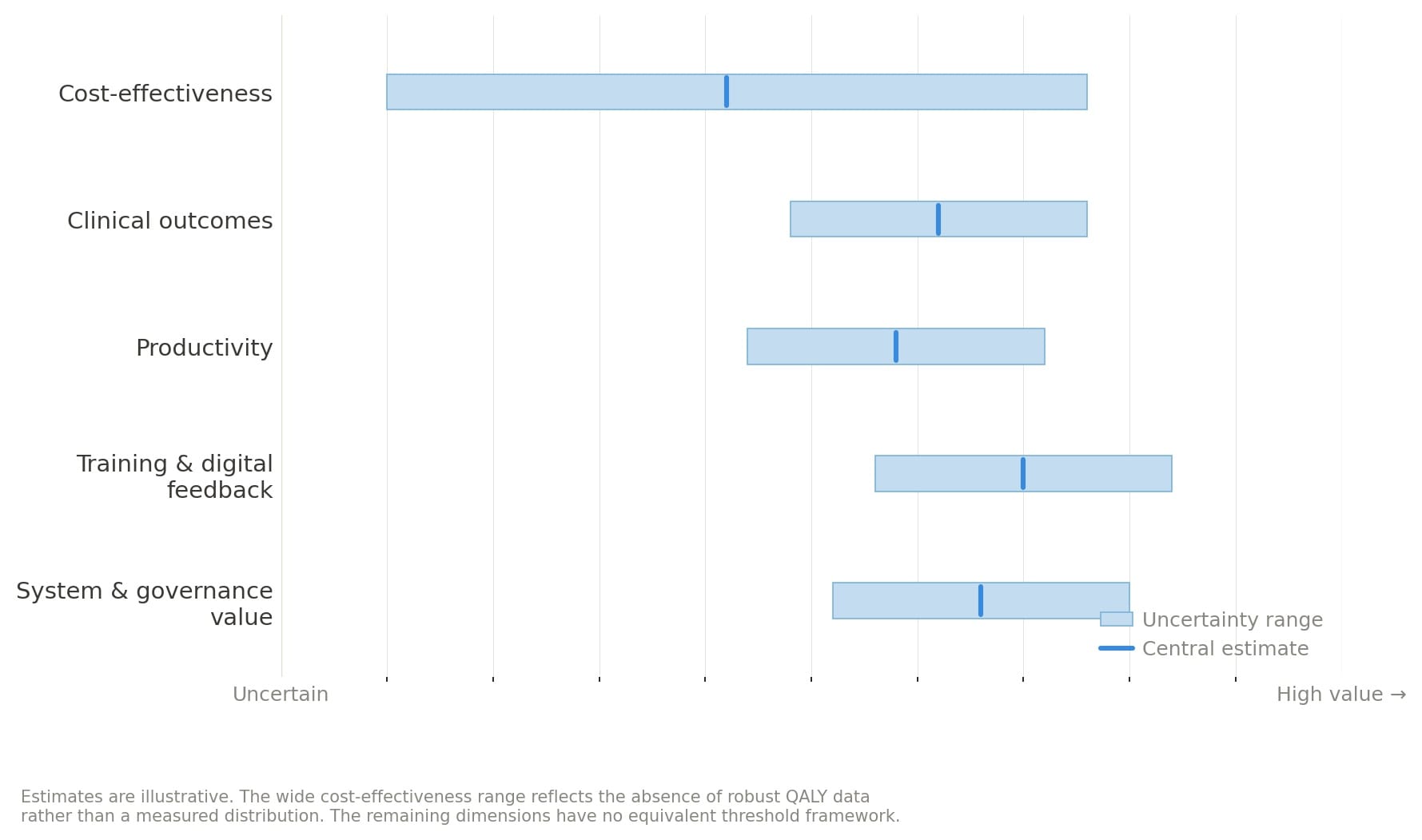
Reframing is therefore needed, and the figure accompanying offers one approach. When robotic surgery is assessed across five dimensions of value, including clinical outcomes, productivity, training and digital feedback, system and governance value, and cost-effectiveness, the last carries the widest uncertainty band of any domain, while the others show a more consistently positive signal that existing frameworks are not equipped to measure. A value compass of this kind does not constitute an argument for uncritical adoption, and it would be a misreading of this editorial to treat it as such. It suggests structured outcome collection, transparent programme-level reporting, and a genuine institutional commitment to generating the evidence that a richer evaluative framework would require. What it rejects is the reduction of that framework to a single threshold designed for a pharmaceutical in an individual patient.
Conflict of interest statement: None declared.
Corresponding author: Professor Aneel Bhangu, Director, Surgical Data Institute, University of Birmingham, UK. a.a.bhangu@bham.ac.uk
References
- Jayne DG, Thorpe HC, Copeland J, Quirke P, Brown JM, Guillou PJ. Five-year follow-up of the Medical Research Council CLASICC trial of laparoscopically assisted versus open surgery for colorectal cancer. Br J Surg 2010; 97: 1638-1645.
- Yaxley JW, Coughlin GD, Chambers SK, et al. Robot-assisted laparoscopic prostatectomy versus open radical retropubic prostatectomy: early outcomes from a randomised controlled phase 3 study. Lancet 2016; 388: 1057-1066.
- Childers CP, Maggard-Gibbons M. Estimation of the acquisition and operating costs for robotic surgery. JAMA 2018; 320: 835-836.
- Jung JJ, Jüni P, Lebovic G, Grantcharov T. First-year analysis of the operating room black box study. Ann Surg 2020; 271: 122-127.
- Sheetz KH, Claflin J, Dimick JB. Trends in the adoption of robotic surgery for common surgical procedures. JAMA Netw Open 2020; 3: e1918911.