Aneel Bhangu, Surgical Data Institute, Department of Applied Health Sciences, University of Birmingham, Birmingham, UK
DOI: 10.5281/zenodo.20491024
Surgical productivity is among the most frequently cited and least precisely defined concepts in NHS management. Trust board papers, elective recovery programmes, and ministerial commitments all discuss it, yet the term is applied interchangeably to lists that begin on time, lists that complete their scheduled cases, and lists that carry sufficient work to justify the allocated session. These are related but distinct properties, and policies designed to improve one can, under the wrong conditions, reliably worsen another. This Analysis article will explore how throughput (the number of operations completed per allocated theatre session) is a more meaningful measure of theatre list productivity than volume alone, and the distinction between the two carries practical consequences that will impact on the current elective recovery programme.
The limitations of alternative metrics are important to consider first:
- Theatre utilisation records the proportion of session time classified as occupied, but says nothing about whether that time produced completed procedures or a succession of delays and abandoned cases.
- Cancellation rate, the figure most routinely reported in NHS performance monitoring, is sensitive to the denominator in ways that make comparisons between lists unreliable: a list cancelling two cases from ten and a list cancelling two cases from six produce the same rate but entirely different outputs.
- Start time compliance reflects only the opening minutes of a session.
- Throughput integrates booking level, cancellation, and case completion into a single figure that corresponds to the outcome that matters to the patient: that the operation was performed.
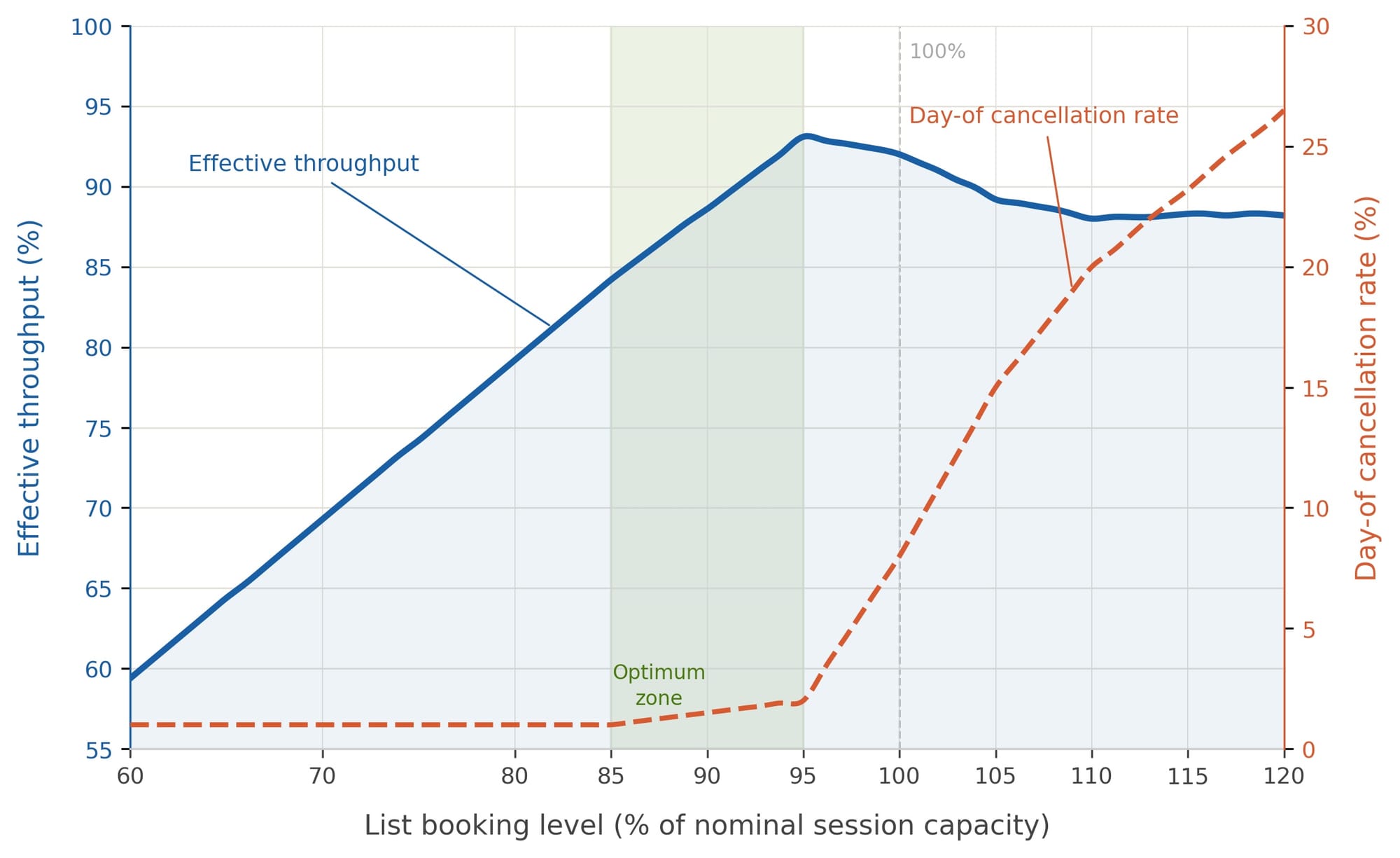
The relationship between booking level and throughput is non-linear, and this sits at the heart of the NHS's current difficulties with elective productivity. As booking levels rise from a low baseline, throughput increases proportionally, with more cases completed and less session time wasted through underuse. This relationship holds until list occupancy approaches somewhere in the region of 85 to 95% of nominal session capacity, at which point throughput is near-maximal and day-of cancellation rates remain low. Beyond this optimum zone, cancellation rates begin to accelerate sharply: the PACE2024 study, a seven-day prospective service evaluation conducted across 91 NHS trusts in November 2024, found a national day-of cancellation rate of 9.9%, with a further 8.7% of patients postponed at preoperative assessment, and one quarter of operating lists running inefficiently1. A list nominally booked at 110% of capacity does not deliver 110% of potential output; the cancellations generated by overbooking consume the margin that additional booking was intended to exploit, and effective throughput falls below that of a well-managed list operating at 90%.
Where a list is running at 75 to 80% of capacity, the operationally appropriate response is to fill the residual session time with short, straightforward day-case procedures that can be completed safely within the available window. This requires departmental infrastructure that most NHS surgical units do not currently maintain. A specialty-level reserve pool of pre-assessed, short-duration day-case patients, held collectively rather than by individual consultants, would allow residual session capacity to be filled at short notice without pushing booking levels into the range at which cancellations accelerate. GIRFT guidance already recommends establishing pools of pre-assessed low-risk patients to support agile scheduling2, and the PACE2024 authors cite early screening and flexible scheduling among their ten priority recommendations for reducing pathway disruption1. The practical reality of doing this routinely has proved very hard for the NHS, for reasons that include pre-operative screening and, understandably, patient availability at the last moment.
The nature of the NHS waiting list itself also requires clarification in this context. At the end of November 2025, there were 7.3 million incomplete referral-to-treatment pathways in England3, a figure routinely characterised in political and media discourse as a surgical waiting list. The referral-to-treatment pathway captures the complete journey from GP referral to first treatment, and the majority of open pathways at any given moment represent patients awaiting a first outpatient appointment, a diagnostic investigation, or a clinical decision rather than an operative admission. In February 2025, only 15.9% of those recorded on the waiting list had a documented decision to admit for treatment4, meaning that fewer than 1.2 million of the total open pathways at that time corresponded to patients for whom a surgical admission had been agreed. Strategies directed at theatre productivity, however effectively implemented, address a minority of the total backlog; the upstream majority requires investment in outpatient capacity, diagnostic throughput, and referral management that operates largely independently of what happens in theatre.
Within the surgical waiting list proper, the scale of accumulation in certain specialties has moved beyond what session-level optimisation can address in isolation. Trauma and orthopaedics carries the largest surgical waiting list in England, and incremental improvements in individual list efficiency, however well sustained, are arithmetically insufficient against a backlog of this magnitude. Structural responses are required alongside session-level discipline: ring-fenced surgical hubs with protected elective capacity, systematic expansion of day-case conversion, and care pathways designed from the outset around volume. Non-clinical last-minute cancellation rates fell substantially following the 2002 national policy intervention, with an interrupted time series analysis demonstrating rapid reductions in both cancellation rates and 28-day breach rates after the penalty policy was introduced, effects that were sustained for many years before being reversed by the COVID-19 pandemic5. The PACE2024 data make clear, however, that once clinical and patient-related cancellations are included alongside non-clinical ones, aggregate day-of cancellation rates remain far higher than headline performance figures suggest, and the gap between reported activity and completed operations is correspondingly large.
| Throughput rate ≥90% | Completion rate <90% | |
|---|---|---|
| Utilisation ≥90% | Productive | Overbooked: patients cancelled, quality at risk |
| Utilisation <90% | Underfilled: session capacity wasted | Failing on both measures |
Completed cases per allocated session, tracked consistently at specialty level and disaggregated by booking level, is the number that reflects what surgical services actually produce. Throughput is the more defensible measure of theatre list productivity than volume, and elective recovery programmes built on occupancy rates and activity counts rather than this metric will continue to mistake scheduling for output. Throughput would need to be presented alongside theatre utilisation, leading to an accurate productivity metric. The optimum booking zone exists, the evidence for it is accumulating, and working deliberately within it is achievable without additional resource, provided that the right number is being tracked. Reliability with throughput and utilisation >90% is better than 99-110% with a 10% cancellation rate.
Cancellations are bad for patients and time consuming for systems, and should be avoided at all costs. Even under these conditions, same day cancellations for reasons of inadequate preoperative preparation require better targeted processes across the whole NHS; cancellations for time should become rare events.
Conflict of interest statement: None declared.
Corresponding author: Professor Aneel Bhangu, Director, Surgical Data Institute, University of Birmingham, UK. a.a.bhangu@bham.ac.uk
References
- Bedford J, McCone E, Hunt A, et al. The Postponement and Cancellations in Elective Care study: a national evaluation of case postponements and cancellations in elective surgical pathways. Br J Anaesth. 2026. doi:10.1016/j.bja.2026.02.034
- Getting It Right First Time. GIRFT resources support findings of national evaluation of surgical postponements and cancellations. London: GIRFT; 2025. Available from: https://gettingitrightfirsttime.co.uk/girft-resources-support-findings-of-national-evaluation-of-surgical-postponements-and-cancellations/
- NHS England. Consultant-led referral to treatment waiting times: statistical press notice, November 2025. London: NHS England; 2026. Available from: https://www.england.nhs.uk/statistics/statistical-work-areas/rtt-waiting-times/
- Nuffield Trust. Why is the planned care waiting list coming down and what does the data really tell us? London: Nuffield Trust; 2025. Available from: https://www.nuffieldtrust.org.uk/news-item/why-is-the-planned-care-waiting-list-coming-down-and-what-does-the-data-really-tell-us
- Quinn L, Bird P, Hofer TP, Lilford R. Cancelled elective operations and 28-day breaches in the NHS in England: an interrupted time series analysis of the 2002 penalty policy, 2008 recession, and COVID-19 pandemic (1994–2023). Lancet Reg Health Eur. 2025;56:101368. doi:10.1016/j.lanepe.2025.101368