
Aneel Bhangu, Surgical Data Institute, Department of Applied Health Sciences, University of Birmingham, Birmingham, UK
DOI: 10.5281/zenodo.20591598
On 17 May 2026, the World Health Organisation declared the Ebola outbreak in the Democratic Republic of Congo a public health emergency of international concern. Caused by the Bundibugyo strain, for which no approved vaccine or treatment currently exists, the outbreak had already crossed into Uganda by the time of that declaration, with suspected cases exceeding a thousand. A four-week gap between the index case’s symptom onset and laboratory confirmation was obscured by co-circulating arboviruses in a healthcare system long strained by conflict.
The situation is familiar, not in the sense that Ebola is routine, but in the sense that the challenge it poses to healthcare systems has been faced before and, in one remarkable instance, answered well.
During the 2014-2016 West African outbreak, Sierra Leone lost effective control of its health system. Hospitals closed or drastically curtailed activity as Ebola moved through clinical environments, killing staff and patients indiscriminately. Across the country, non-Ebola surgical admissions fell by more than half, and the indirect mortality from trauma unattended, appendicitis untreated, and emergency obstetric conditions turned away was substantial and largely uncounted.
One hospital, at Goderich on the western edge of Freetown, remained open. It sat in the Western Area of Sierra Leone, which ultimately accounted for 41% of all nationally confirmed cases, and it recorded zero healthcare worker infections across 406 staff over twelve months. As the internationally recognised non-governmental organisation EMERGENCY published their data1, it provided the formal account of how that was achieved, and it is worth reading carefully while the DRC outbreak is active and hospital preparedness is once again a live question.
EMERGENCY is an Italian humanitarian NGO founded in 1994 by the surgeon Gino Strada, built on the conviction that high-quality medical care is a universal right rather than a geographically contingent privilege. Its surgical hospitals operate free of charge in conflict and humanitarian settings across Afghanistan, Sudan, Sierra Leone, and Uganda, and its record is one of sustained clinical quality under conditions that would close most institutions. In Goderich, it had been running the only free surgical hospital in Sierra Leone since 2001, and it was that institutional culture of preparation, of commitment to remaining open, and of investment in local staff that shaped its Ebola response.
The intervention was comprehensive and, critically, early. EMERGENCY mobilised before Sierra Leone’s official outbreak declaration, having monitored transmission in neighbouring Guinea for months. The hospital was reorganised around what the paper describes as a “four-dimensional logic”, controlling the movement of people, places, items, and time to minimise every route of transmission. A dedicated screening area was established outside the main building. Screening nurses were selected specifically for their familiarity with local customs, a deliberate choice in a context where stigma caused patients to conceal risk factors and where common paediatric presentations overlapped substantially with early Ebola virus disease symptoms. Staff received a salary increase of 25% for the duration of the epidemic and were required to work exclusively at the EMERGENCY facility. Educational programmes were extended to staff families and communities. Attention to staff welfare was crucial: healthcare workers experienced disproportionately high Ebola-related mortality during the early phases of the epidemic and could themselves become important vectors of transmission if inadequately protected.
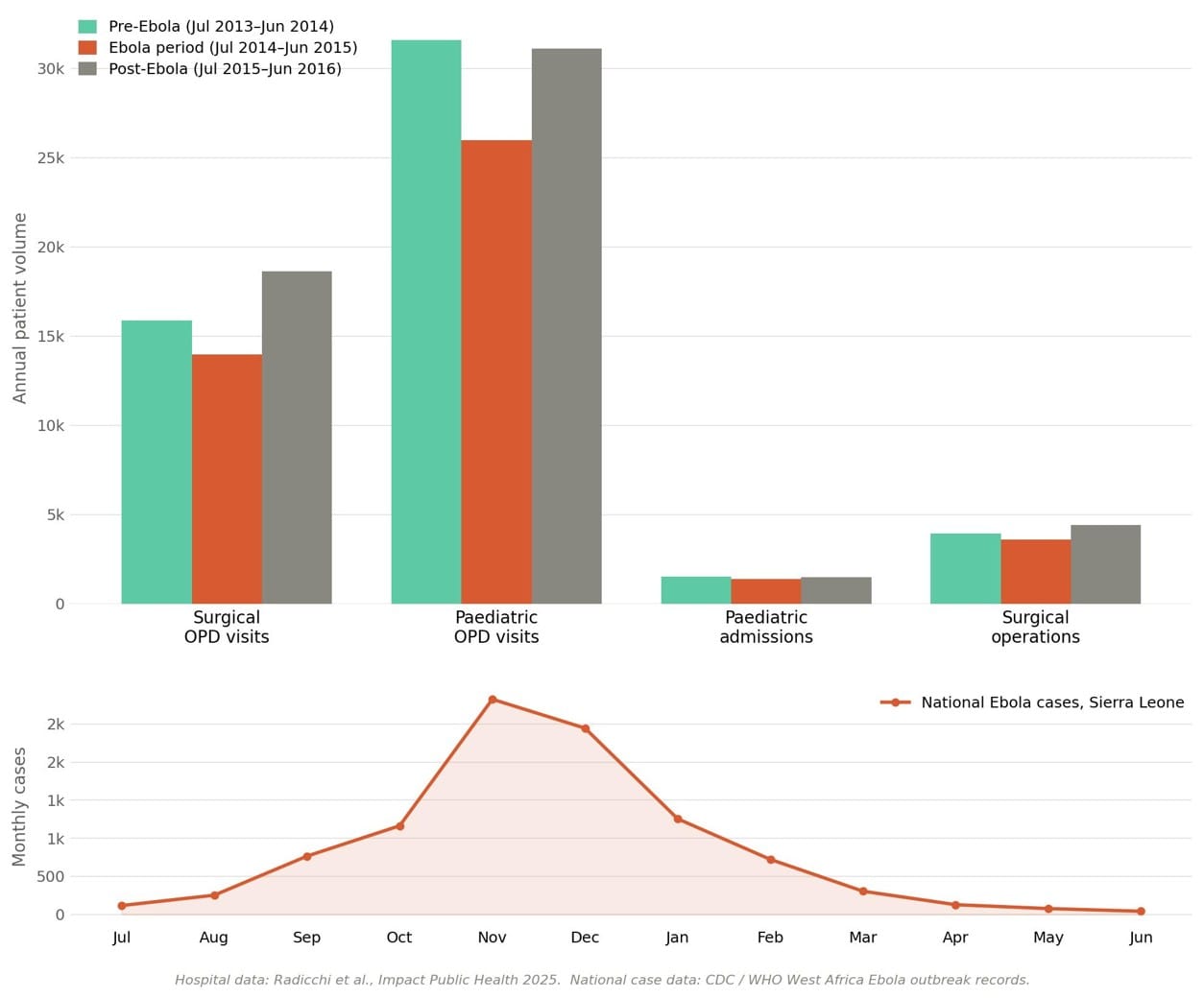
During the twelve-month outbreak period, 31,473 individuals were screened, 19 confirmed cases were identified and transferred to an Ebola Treatment Centre, and one surgical emergency confirmed as Ebola-positive was managed in an isolation unit without secondary transmission. Surgical operations fell by 9.1% compared with the pre-outbreak period and paediatric admissions by 9.6%, reductions that reflected fear-related barriers to attendance rather than any withdrawal of clinical capacity. In the subsequent year, surgical activity exceeded its pre-Ebola baseline by 12%.
What the Goderich experience demonstrates, and what the 2026 DRC outbreak makes relevant again, is that the reflexive closure of hospitals during an epidemic is not the only possible response. Timeliness, systematic infection control, genuine investment in staff welfare, and institutional leadership willing to treat an epidemic as an operational systems problem before it arrives rather than a crisis to be managed after it does. The indirect harm from surgical access collapse is diffuse and difficult to measure, but it is real, and it falls on patients who have no alternative. In Goderich between 2014 and 2015, EMERGENCY demonstrated that those patients need not be abandoned. That demonstration has not aged.
About EMERGENCY ONG ETS
EMERGENCY was founded in Milan in 1994 by the trauma surgeon Gino Strada, following his years’ operating with the International Committee of the Red Cross in Afghanistan, Somalia, Ethiopia, and Bosnia. Its founding premise that access to high-quality medical care is a fundamental human right, not a privilege determined by geography or income) has guided three decades of work across conflict zones and humanitarian emergencies.
The organisation has treated more than 12 million patients to date. It currently operates surgical hospitals and medical centres across Afghanistan, Eritrea, Iraq, Italy, Sierra Leone, Sudan, and Uganda, providing all care entirely free of charge. Its facilities range from frontline trauma centres for war-wounded patients in Kabul and Lashkar-Gah to the Salam Centre for Cardiac Surgery in Khartoum, the only completely free cardiac surgery hospital serving a population of more than 300 million people across sub-Saharan and East Africa. Opened in 2007 and a recipient of the Aga Khan Award for Architecture, the Salam Centre has performed more than 10,000 cardiac operations and drawn patients from 33 countries across Africa, the Middle East, and Asia. In Uganda, EMERGENCY’s Children’s Surgical Hospital in Entebbe extends this model of specialist surgical excellence to paediatric care.
In Sierra Leone, EMERGENCY has operated the Goderich Surgical and Paediatric Centre in Freetown since 2001, when it opened at the end of the country’s civil war as the only free surgical hospital in the country. The centre serves as the national referral centre for orthopaedics and traumatology and has maintained continuous operations through successive crises, including the 2014–2016 Ebola outbreak and the COVID-19 pandemic. Sierra Leone’s Ministry of Health and Sanitation recognised it as the Best Performing Medical Emergency Response Team for its conduct during both. During the most critical period of the outbreak, from mid-2014 to May 2015, EMERGENCY also operated separate services for Ebola-affected patients in the same region, helping preserve continuity of care while limiting cross-transmission risks.
EMERGENCY’s model is deliberately permanent rather than expeditionary: it builds facilities, trains local clinical staff to the highest professional standards, and embeds itself within the communities it serves for the long term. Gino Strada, who died in August 2021, described the organisation’s purpose as proving that quality medicine is possible anywhere. Its record, accumulated across 30 years and more than a dozen countries, constitutes the most sustained demonstration of that argument in the history of humanitarian surgery.
Conflict of interest statement: None declared.
Corresponding author: Professor Aneel Bhangu, Director, Surgical Data Institute, University of Birmingham, UK. a.a.bhangu@bham.ac.uk
References
- Radicchi L et al. Protecting a healthcare facility during the Ebola outbreak: preparedness, mitigation, and continuity of care in Sierra Leone. Impact Public Health 2025; 1(1): 1–8.