Professor Aneel Bhangu, Professor of Colorectal Surgery, Surgical Data Institute, University of Birmingham, UK
Professor Simon P Bach, Professor of Colorectal Surgery, University of Birmingham, UK and Vice chair of the NICE Interventional Procedures Advisory Committee
Professor Deena Harji, Associate Professor of Surgery, Clinical Trials Research Unit, University of Leeds and Consultant Colorectal Surgeon, Manchester University NHS Foundation Trust, UK
DOI: 10.5281/zenodo.19237219
Robotic-assisted surgery (RAS) is being implemented at a pace, challenging the capacity of our health systems to appraise its long-term value. In April 2025, the UK’s National Institute for Health and Care Excellence (NICE) opened an Early Value Assessment (EVA) pathway to help meet this challenge, resulting in conditional approvals and 3 year window for evidence generation to address specific evidence gaps. The conditional approvals were for 11 robotic platforms (five soft tissue and six orthopaedic), on a path that allows new health technologies that do not have a complete evidence base to be used within the NHS while evidence generated. This dual signal (implementation and conditional approval) illustrates the tension between technological momentum and, in formal terms, an unproven health economic case. The 3 year timeline for evidence generation puts an onus on industry collaboration for this first phase, probably signalling the need for a full evidence base of early, mid-term, and late clinical outcome and quality of life data.
The soft-tissue surgical-robotics market was US$10.4bn in 2024 and, after adjusting for a gradual, non-explosive rise in robotic procedure share, is projected to reach US$20.7bn by 2030 under the baseline scenario. This procedure-adjusted framework models year-by-year growth as a steady base rate with a small, linear uplift each year, reflecting robotics’ incremental replacement of laparoscopy. The forecast band spans US$18.2-24.0bn by 2030 across conservative to optimistic tracks, with a 2025 baseline checkpoint of ~US$11.6bn.
Figure 1. Global soft-tissue surgical-robotics spending (company-anchored, procedure-adjusted): observed (2020–2024) and forecast scenarios (2025–2030).
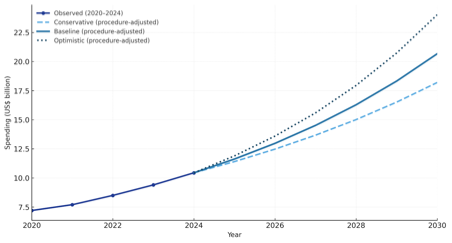
Scope is soft-tissue only and includes systems, instruments & accessories, and services. The 2024 base is US$ 10.44 bn, derived from Intuitive Surgical’s 2024 revenue (US$ 8.35 bn) assuming ~80% share of soft-tissue spend. Annual growth uses a year-by-year rate equal to a scenario base rate plus a small, linearly rising uplift that reflects increasing robotic procedure share as robotics displaces laparoscopy (medium, cautious). Line styles: Baseline solid, Conservative dashed, Optimistic dotted. Key checkpoints (USD bn): 2025 baseline = 11.62; 2030 = 18.19 / 20.66 / 24.02 (conservative / baseline / optimistic).
Robotics has become a strategic priority for the current leadership of the UK’s Department of Health and Social Care (DHSC). The NHS 10-Year Plan (2025) includes a stated ambition for robotic systems to support up to 90% of keyhole surgery by 2035, a substantial increase from approximately 1 in 60 operations today. Secretary of State Wes Streeting reaffirmed this goal in June 2025. Sir Jim Mackey, NHS Chief Executive, has further clarified that this equates to approximately 12.5% of all surgery being robot-assisted by 2035. DHSC expects the volume of robotic procedures to rise to 500,000 annually by 2035. The NICE HealthTech Evaluation programme has been repositioned as the lead assessment pathway for emerging surgical technologies, feeding directly into purchasing guidance for Integrated Care Systems. In April 2025, NICE’s Early Value Assessments HTE21 and HTE22 recommended urgent real-world studies addressing “priority evidence gaps” in robotic surgery and requested large prospective cohorts with linked quality-of-life data. NICE also cited concerns about geographic inequality, with most robotic centres concentrated around major urban hospitals; NBOCA data demonstrate up to a 30% difference in availability of RAS across the least and most deprived areas in the UK.
The scale and spending necessary to achieve both robotic coverage and excellence in the NHS might not be as vast as some imagine, compared to whole health budgets. This is revealed by exploring the current and projected costs of RAS in the context of wider surgical budgets and whole healthcare budgets. The NHS in England undertakes surgery for roughly 4.4 million people per year, while Hospital Episode Statistics record around 12.4 million consultant episodes with at least one procedure; about 70,000 robotic procedures were performed in 2023/24. On headline figures from our NHS analysis (contained within this journal issue), a middle view puts programme spend at around £0.30 bn at year 5 with a plausible range of ~£0.06–0.61 bn, equating to ~0.14% of the NHS budget (~0.03–0.29%). By year 10, spend settles near £0.20 bn (~£0.05–0.41 bn) or ~0.09% of the NHS budget (~0.02–0.18%). Over a decade, the cumulative envelope is ~£2.0 bn (~£0.48–4.11 bn). This amount will be further reduced by offset laparoscopy costs, which are already built into spending. Although the total budgetary impact on the wider NHS is low, future governments are still likely to ask for evidence to justify decisions to taxpayers and support ongoing spending.
Randomised trials between robotic and laparoscopic surgery will prove challenging for many indications, as robotic implementation is already widespread and robotic surgeons are unlikely to step back to laparoscopy, especially whilst on their learning curves. However, clinical equipoise remains for several procedures and specialties. Without structured real-world evaluation, robotic implementation risks undermining value-based policy by increasing costs without proportional or proven clinical benefit. The roll of other aspects of improvement, such as training, access to digital data, exclusion of rare outlying negative events, may be harder to measure but just as important. Team productivity from a focussed robotics list may be an even greater additional benefit, that deserves measurement. Whether high performing teams can be replicated everywhere, or need to be amplified where they are successful, is yet to be seen. There is now a perfect opportunity to generate prospective data to inform the use of robotic platforms across indications, technologies, and geographies.
This call to evidence is particularly important for national systems such as the NHS, which operate under centralised budgets and where investment decisions must be population-based. In contrast, robotics uptake in the United States is likely to continue without constraint, driven by fee-for-service incentives and hospital-level marketing. US installations have surpassed 6,000 da Vinci systems, with widespread uptake across academic and private hospitals. Middle-income countries, where procurement is often donor- or industry-led, remain in an exploratory phase. In these settings, the absence of outcome data and the scale of operating costs may prevent long-term adoption in public systems. A recent commentary noted that in low- and middle-income countries, robotic procurement, often via public-private partnerships, may exceed long-term budgets without efficiency gains.
The robotic market has started to diversify over the last five years. While da Vinci systems continue to dominate, new entrants including Versius, Hugo, and Senhance have expanded availability. Hybrid platforms, combining laparoscopic and robotic elements, are gaining traction, especially where cost is a concern. Still, there remains a severe lack of national comparator study, and registry efforts, while valuable, do not offer the speed and design features required for unbiased evaluation. The NIHR-funded REINFORCE study will begin to fill this gap, reporting early findings by late 2025.
A formal evidence strategy is therefore essential, encompassing prospective procedure level cohorts with contemporary comparison to laparoscopy, incorporating quality of life endpoints and long term follow up, and powered individually for procedures where genuine equipoise remains, including colon resection, hysterectomy, liver resection, lung resection, inguinal hernia repair, and cholecystectomy. This should be complemented by descriptive and comparative analyses across multiple platforms, including at least those identified within NICE HTE21 and HTE22, alongside the development of geographic equity metrics to assess implementation across all regions, including within centres that already possess robotic capability. In parallel, detailed health economic scenario modelling using NHS specific data will be required to understand system level implications, while a pragmatic and comprehensive evaluation of learning curves at the level of the surgeon, the wider operative team, and the hospital should be undertaken, explicitly linked to real world clinical and organisational outcomes.
In the long term, public systems will demand different types of evidence than investor-driven markets and we should prepare for this now. After the current five-year window, ongoing research for learning curve impact and productivity, especially at team level, will help support ongoing investment and realise ambitions that surgeons, governments, and patients want, albeit with proven value.
Corresponding author: Professor Aneel Bhangu, Director, Surgical Data Institute, University of Birmingham, UK. a.a.bhangu@bham.ac.uk
Previously published as: Bhangu, A., Bach, S. and Harji, D. (2025) “Robotic surgery: A call for evidence in value-based health systems”, Impact Surgery, 2(7), pp. 223–225. doi: 10.62463/surgery.264.
References
- National Institute for Health and Care Excellence. Robot-assisted surgery for soft tissue procedures: early value assessment (HTE21). 2025 Apr 17 [cited 2025 Aug 31]. Available from: https://www.nice.org.uk/guidance/hte21
- MarketsandMarkets. Surgical Robots Market by Product, Application, End User – Global Forecast to 2029. 2024 [cited 2025 Aug 31]. Available from: https://www.marketsandmarkets.com/Market-Reports/surgical-robots-market-256618532.html
- Intuitive Surgical Inc. Q2 2025 Investor Report and Earnings Call. Sunnyvale (CA): 2025 Jul [cited 2025 Aug 31]. Available from: https://isrg.gcs-web.com/static-files/b75d10ff-8f60-4f52-bd1a-2b2b2fc78a83
- Watson SL, Fowler AJ, Dias P, et al. The lifetime risk of surgery in England: a nationwide observational cohort study. Br J Anaesth. 2024;133(4):768–75.
- NHS England. Provisional Monthly Hospital Episode Statistics for Admitted Patient Care, Outpatient and A&E, Apr 2023–Feb 2024. Published 2024 Apr 11. Available from: https://digital.nhs.uk/data-and-information/publications/statistical/provisional-monthly-hospital-episode-statistics-for-admitted-patient-care-outpatient-and-accident-and-emergency-data/april-2023---february-2024
- NHS England. Millions to benefit from NHS robot drive. 2025 Jun 11 [cited 2025 Aug 31]. Available from: https://www.england.nhs.uk/2025/06/millions-to-benefit-from-nhs-robot-drive/
- Canadian Agency for Drugs and Technologies in Health. Da Vinci Robotic Surgical System: Review of Clinical and Cost Considerations. Ottawa: CADTH; 2011. Report No.: L0052.
- NICE. Robot-assisted surgery for soft tissue procedures: Early Value Assessment (HTE21) – Summary. 2025 Apr 17. Available from: https://www.nice.org.uk/advice/hte21/chapter/Summary
- Department of Health and Social Care. 2024 to 2025 revised financial directions to NHS England. 2025 Mar 31. Available from: https://www.gov.uk/government/publications/2024-to-2025-revised-financial-directions-to-nhs-england
- Aggarwal A, Han L, Boyle J, et al. Association of quality and technology with patient mobility for colorectal cancer surgery. JAMA Surg. 2023;158(1):e225461.
- Burke J, Gnanaraj J, Dhanda J, et al. Robotic surgery in low- and middle-income countries. Bull R Coll Surg Engl. 2024;106(3):138–41.
- NIHR Applied Research Collaboration North East and North Cumbria. REINFORCE – A real-world, in situ evaluation of the introduction and scale-up of robot-assisted surgical services in the NHS. 2025 [cited 2025 Aug 31]. Available from: https://arc-nenc.nihr.ac.uk/projects/reinforce-a-real-world-in-situ-evaluation-of-the-introduction-and-scale-up-of-robot-assisted-surgical-services-in-the-nhs