Professor Deena Harji, Associate Professor of Robotic Surgery, Manchester University NHS Foundation Trust and University of Leeds, Manchester, UK
DOI: 10.1038/s41586-026-10796-x
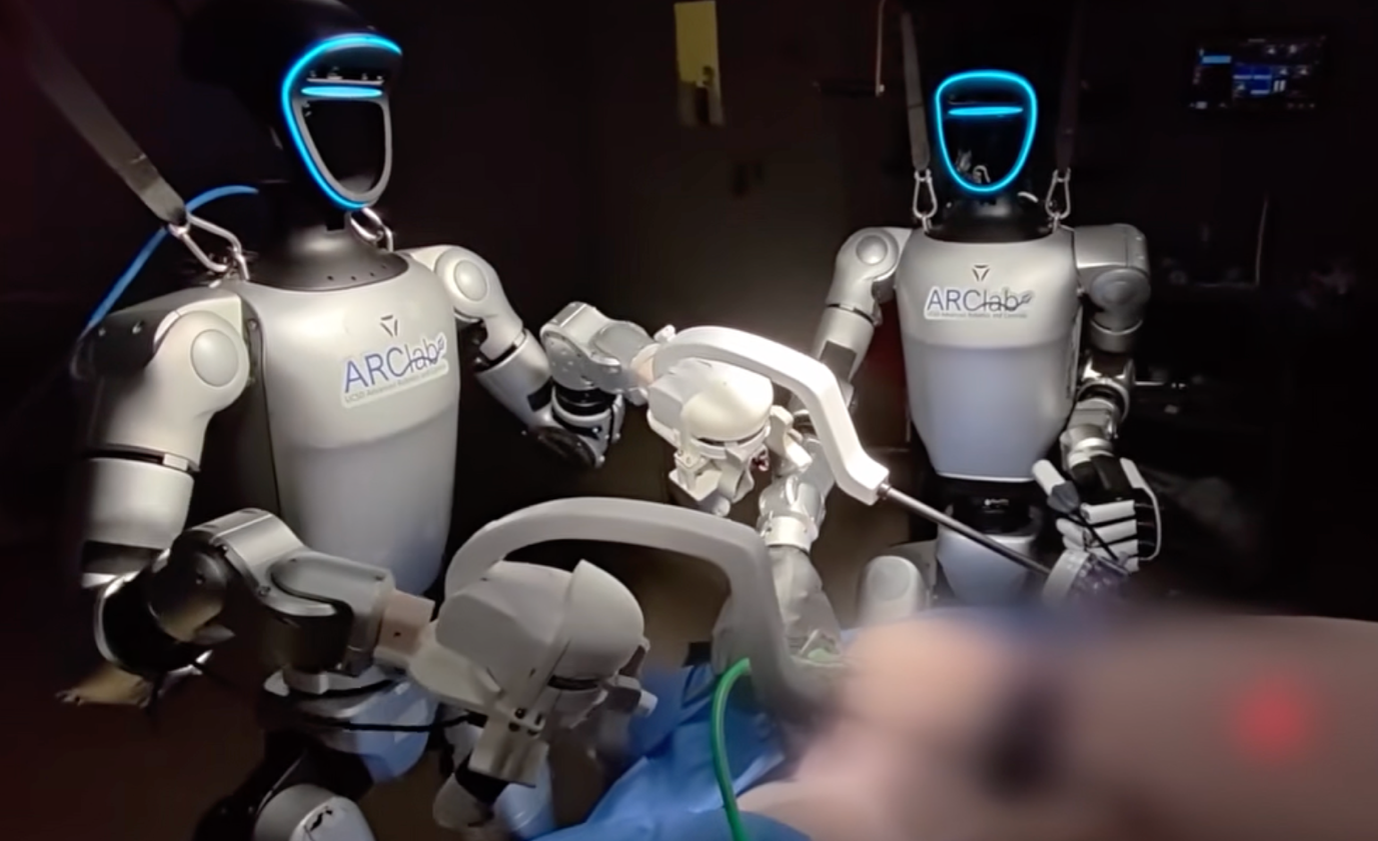
Last Wednesday, I was sat at London City Airport waiting to board my flight to Luxembourg for the inaugural TROGGS (The Robotic Global Surgical Society) meeting, gazing across the blue London sky, seeking inspiration to write my talk on ‘Multidisciplinary Robotic Surgery’. As I let procrastination take over, inspiration came from the formidable Professor Michael Yip, who had just posted on LinkedIn about his breakthrough experiment on a teleoperated humanoid robot successfully performing laparoscopic surgery in a preclinical animal model. It is undoubtedly an impressive technical achievement and one that deserves due recognition. His YouTube video made it straight onto my opening slide and was the source of much thought-provoking discussion both at the TROGGS meeting, but also throughout social media networks over the last few days. Elon Musk’s prophecy had been realised, surgeons are going to be replaced by humanoid robots and its didn’t even take the predicted 3 years!
The global humanoid robot market size was valued at USD 4.89 billion in 2025 and is projected to reach USD 165.13 billion by 2034, with Asia Pacific dominating the market share. Humanoids are designed to be human-like, with an aim to seamlessly integrate into our environment and existing infrastructure. It therefore is, really no surprise, that they are entering the healthcare arena, with the promise of automating repetitive labour intensive or physically demanding tasks, addressing workforce shortages, and improving efficiency and productivity. The NHS is facing unprecedented workforce and productivity pressures, with the NHS Long Term Workforce Plan projecting the need for up to 300,000 additional healthcare staff by 2036, all whilst demand for services continues to increase. By 2030, over 11 million people in England will be aged over 65, increasing demand for surgical care, rehabilitation, and community services. These pressures are reflected in system capacity challenges, with more than 7 million people currently on NHS waiting lists. Could humanoids be the answer? National policy increasingly emphasises automation and digital transformation as key enablers of healthcare productivity, including plans to expand robotic technology within the NHS. A closer look at the NHS 10-year plan reveals its ambitions beyond scaling robotic-assisted surgery, to include pharmacy automation, hospital logistics robotics, and rehabilitation/assistive robotics to reduce workforce pressures and improve efficiency. There are already siloed examples of these robotic technologies cropping up within the NHS, with examples of pharmacy automation, hospital logistics robots using automated guided vehicles that move food, linen, medicines and supplies, and rehabilitation robotics for stroke rehabilitation. So, perhaps it’s time to assess how humanoid technology can be introduced into the NHS operating theatre?
There are many interesting things about Michael Yip’s study, including, the use of a commercially available humanoid robotic system, the Unitree G1 humanoid system, the decision to perform a laparoscopic cholecystectomy, which is one of the commonest general surgical operations globally, and the teleoperation framework, retaining the human-in-the-loop; demonstrating that this really is a collaboration between human surgeons and humanoid robots. These key design decisions provide a realistic insight into how this technology could cross-over and be deployed into real world clinical practice. And, although, this study demonstrates the feasibility of humanoid robots manipulating laparoscopic instruments to execute a common surgical procedure, it highlights several limitations, including increased operative time, disruptions in workflow due to humanoid robot recalibration and reposition, teleoperation latency and reduced dexterity and reach compared to traditional robotic systems.
Beyond the sensationalised headlines, this study is likely to be the first of many navigating the path from engineering readiness to clinical deployment within the operating room. Whilst engineering refinements are required to facilitate clinical implementation, other key parallel questions will need to be answered by the clinical and academic community, including, clinical and cost-effectiveness, governance and oversight, ethical and legal implications. Ensuring the development of upfront clinical and implementation frameworks for initial deployment, alongside mapping out procedural indications and workflows will be paramount to the success of the humanoid surgeon, ensuring the right operation is performed by the right surgeon and clinical team and the right robot.
The future diversification of the robotic landscape will extend beyond the current range of traditional telemanipulator platforms, and will likely include autonomous systems, AI-guided systems and humanoid systems, each with their own set of indications, benefits and limitations. Aligned to this, we will need to develop regulatory, legal and governance frameworks to safeguard patients, maintain high quality standards of clinical care and support the surgeons and clinical teams employing these systems. It is clear that we will be operating in an increasingly complex surgical/robotic/engineering arena in the future. This is, perhaps best highlighted by the fact that, 30 days prior to the publication of the Yip study, the The U.S. Department of Defense added Unitree to its Section 1260H list of Chinese military-affiliated companies, following an independent and comprehensive security audit. This found that G1 continuously transmits data to servers in China every five minutes without notifying the operator and without any consent mechanism. The transmitted data includes battery status, joint torque, motion state, and sensor information from the robot's cameras, microphones, and internal services (audio and video feeds), spatial data, and GPS location. The other significant vulnerability was the "UniPwn" exploit, which demonstrated that the robot operates with hardcoded encryption keys, allowing hackers within Bluetooth range to escalate to root privileges. Once compromised, the robot could automatically propagate the infection to other susceptible units nearby, creating a self-propagating robot botnet. Clearly, this raises an important question regarding cybersecurity and geopolitical vetting of such systems. The NHS digital infrastructure and health data security are core elements of UK national security strategy, with the Cyber Security and Resilience Bill establishing stringent cybersecurity standards for the healthcare sector. However, there are growing concerns, that existing standards and product liability frameworks are not fully equipped for the complexities of humanoid robots, particularly with regards to their network-connected nature and autonomous decision-making. There is a clear need for regulation to evolve alongside technological innovation to facilitate timely implementation of new healthcare technologies.
There is obviously a human angle to teleoperated humanoid robotic surgery, both from a surgical and patient perspective. Proponents of humanoid robotic surgery will argue that the use of teleoperation retains the surgeons’ judgment and dexterity whilst relocating their surgical skills, transferring these through a console to the humanoid robotic system to execute an operation. Sceptics will argue that there is an art to the science of surgery, beyond the technical execution requires judgement, complex decision-making, team work and communication; replacing humans with humanoids is a technical exercise, and does not reflect the realities of surgery. Perhaps, more important than both of these surgical perspectives, is the patient perspective, will patients be willing to undergo teleoperated humanoid robotic surgery? There are clear issues around consent, safety, accountability and liability that will need to be addressed, and our patients will need to be sufficiently reassured of the safety of this approach in the future.
Is the NHS ready for humanoid robotics, probably not today, but as a surgical community, this latest paper provides us with plenty of food for thought for what the future could look like. If the current trajectory of robotics, embodied AI, and foundation models continues, humanoid robots could evolve into intelligent members of the healthcare team. Will they replace surgeons? It’s very unlikely, but I suspect, they will be become part of the wider multidisciplinary healthcare team, with their role being to support and augment. It’s an exciting time for our profession, and I am looking forward to extending my multidisciplinary team with a humanoid team member.
Conflict of interest statement: None declared.
Corresponding author: Professor Deena Harji, Associate Professor of Robotic Surgery, Manchester University NHS Foundation Trust and University of Leeds, UK. deena.harji@nhs.net
Full paper: Liang, Z., Thareja, N., Zhang, P. et al. In vivo feasibility study of humanoid robots in surgery. Nature (2026). https://doi.org/10.1038/s41586-026-10796-x