
João Martins1, Aneel Bhangu1
1Surgical Data Institute, Department of Applied Health Sciences, University of Birmingham, Birmingham, UK
DOI: 10.5281/zenodo.20214918
Colorectal cancer is the fourth most common cancer in the UK, with around 48,200 new cases diagnosed every year.¹ Despite multiple national policies, continuous investment in new technologies, and advances in adjuvant therapeutics, improvements in survival over the last 25 years have only been modest.² Across the NHS, clinical pathways have been established to ensure that patients presenting to primary care have timely access to diagnosis and treatment, a key determinant of patient survival. However, driven by rising demand, system pressures, and the expanding role of personalised medicine, these pathways have become increasingly complex, multiplying the opportunities for delay. Current mechanisms for identifying, monitoring, and investigating these delays remain poorly defined and are typically focused on time to surgery. NHS waiting time targets, whilst operationally useful, lack details on where or why delays occur across modern pathways. As a result, the opportunity for patient level improvement is lost and proposed system level solutions are often misdirected, focusing on surface metrics whilst failing to address the underlying causes. At the same time, existing conceptual models of delay have not been tailored to the complexities of NHS colorectal cancer pathways. In the absence of relevant validated tools, reducing delays across the patient care journey remains difficult and ineffectual.
Why delays matter
The clinical consequences of delays accumulate across the pathways. In primary care, a 2017 pooled analysis of seven cohorts from high-income countries showed that delayed referral to a specialist centre was associated with a higher likelihood of advanced disease at presentation.³ Once referred, delays to diagnosis carry additional risk, illustrated by a 2021 systematic review which found that colonoscopy performed beyond nine months of a positive faecal immunochemical test (FIT) was associated with a higher incidence of stage III or IV colorectal cancer.⁴ Additionally, compounding delays to histology, radiology, and multidisciplinary team meetings are likely to lead to similar outcomes.
Beyond diagnosis, delays in treatment are associated with significant reductions in survival. A meta-analysis by Hanna et al. found a 6% decrease in overall survival for every four-week delay to surgery in colon cancer,⁵ whereas Whittaker et al. reported reductions of 13% and 57% in patients with resectable, non-metastatic colorectal cancer whose surgery was delayed by four and twelve weeks, respectively.⁶ Delays to adjuvant chemotherapy after surgery provides independent risk, with two meta-analyses showing that a four-week delay to its initiation increases mortality risk by 13–14%.⁵˒⁷ However, the relationship between delay and outcome is not always straightforward. A large international prospective cohort study found that surgical delays of up to twelve weeks were not associated with worse rates of complete resection, hypothesising that the impact on survival may be linked to micro-metastatic disease spread rather than local cancer control.⁸
Current landscape
Current NHS waiting time targets in England include the 28-day Faster Diagnosis Standard (FDS, from referral to diagnosis), the 31-day treatment standard (from decision to treat to 'first definitive treatment' initiation), and the 62-day treatment standard (covering the entire referral-to-treatment interval), with similar indicators available in the devolved nations. Whilst useful as performance metrics, these targets have several limitations in characterising delays.
First, they measure endpoints rather than processes, providing no information on the reason behind good or bad performance; delays occurring at specific points throughout the pathways may go undetected. Second, these metrics are heterogeneous, encompassing a wide range of actors and activities. The FDS, for instance, is affected by factors as disparate as referral systems between primary and secondary care, endoscopy and radiology capacity, and patients' financial ability to attend appointments. Third, the targets do not cover all clinically relevant time intervals: the period between primary care presentation and referral, and the interval between surgery and start of adjuvant chemotherapy, are notable omissions. Fourth, they do not consistently distinguish between avoidable delays and clinician-patient initiated pauses. For example, neoadjuvant chemotherapy, unlike surgery, is not considered a 'first definitive treatment' under the 31-day treatment standard, creating a structural blind spot. Fifth, the evidence underpinning the specific metric thresholds (28, 31, or 61 days) is relatively thin. Collectively, these metrics do not tell us where delays actually occur, nor why.
Existing conceptual models of delay are similarly ill-suited to the task. The Three Delays Model, recently extended to Six Delays,⁹ was developed to examine preventable maternal mortality in low and middle-income countries¹⁰ and does not map well onto NHS cancer pathways. Andersen's General Model of Total Patient Delay and Walter et al.'s Model of Pathways to Treatment are rooted in psychological theory and focus predominantly on patient-level delays such as health-seeking behaviours.¹¹˒¹² The Aarhus statement, an international reporting guideline on early cancer research, despite helpfully standardising key time points and intervals, lacks pathway-level granularity (especially at secondary-care level) and is not specific to colorectal cancer or the UK context.¹³
Next steps
The recently published National Cancer Plan for England sets an ambition for three in four patients to survive cancer for five years or more by 2035 and commits to meeting all cancer waiting standards by 2029. However, ambitious targets are unlikely to be achieved without a structured understanding of why these are not met in the first place.
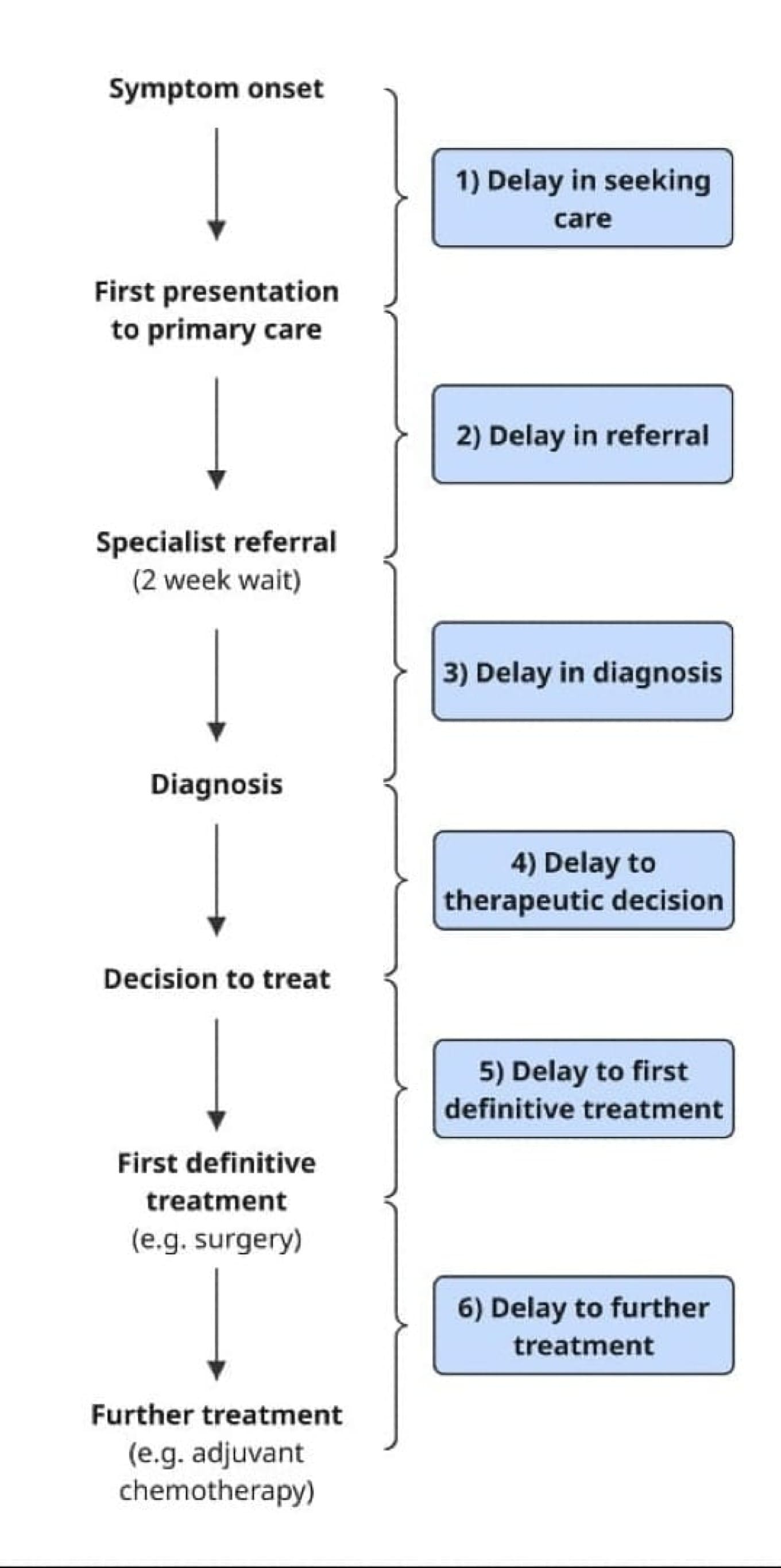
We therefore propose to develop a validated delay framework for the NHS colorectal cancer diagnostic and treatment pathways, anchored in a draft model of six delays (Figure 1) and built through expert consensus. This would provide clinicians, service managers, and policymakers with the tools to identify the root causes of delays and develop targeted interventions to address them. Additionally, having a detailed model of these pathways would strengthen clinical governance, serving as a mechanism to investigate patient complaints and deal with litigation arising from delayed care.
The need for a robust framework of delay that maps colorectal cancer pathways is clear. It is time to create one.
Conflict of interest statement: All authors declare no conflict of interest.
Corresponding author: Dr. João Martins, j.m.martins@bham.ac.uk, Surgical Data Institute, University of Birmingham, Birmingham B15 2TT, UK
Corresponding author: Professor Aneel Bhangu, a.a.bhangu@bham.ac.uk, Surgical Data Institute, University of Birmingham, Birmingham B15 2TT, UK
References
- Cancer Research UK. Bowel cancer statistics. Available from: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/bowel-cancer
- Pedregal-Pascual P, Guarner-Argente C, Tan EH, et al. Incidence and Survival of Colorectal Cancer in the United Kingdom From 2000 to 2021: A Population-Based Cohort Study. Am J Gastroenterol. 2025;120(12):2909–17. doi:10.14309/ajg.0000000000003460
- Tørring ML, Murchie P, Hamilton W, et al. Evidence of advanced stage colorectal cancer with longer diagnostic intervals: a pooled analysis of seven primary care cohorts comprising 11,720 patients in five countries. Br J Cancer. 2017;117(6):888–97. doi:10.1038/bjc.2017.236
- Forbes N, Hilsden RJ, Martel M, et al. Association Between Time to Colonoscopy After Positive Fecal Testing and Colorectal Cancer Outcomes: A Systematic Review. Clin Gastroenterol Hepatol. 2021;19(7):1344–1354.e8. doi:10.1016/j.cgh.2020.09.048
- Hanna TP, King WD, Thibodeau S, et al. Mortality due to cancer treatment delay: systematic review and meta-analysis. BMJ. 2020;371:m4087. doi:10.1136/bmj.m4087
- Whittaker TM, Abdelrazek MEG, Fitzpatrick AJ, et al. Delay to elective colorectal cancer surgery and implications for survival: a systematic review and meta-analysis. Colorectal Dis. 2021;23(7):1699–711. doi:10.1111/codi.15625
- Biagi JJ, Raphael MJ, Mackillop WJ, et al. Association between time to initiation of adjuvant chemotherapy and survival in colorectal cancer: a systematic review and meta-analysis. JAMA. 2011;305(22):2335–42. doi:10.1001/jama.2011.749
- COVIDSurg Collaborative. The impact of surgical delay on resectability of colorectal cancer: An international prospective cohort study. Colorectal Dis. 2022;24(6):708–26. doi:10.1111/codi.16117
- Franke MA, Pasteur GI. The Six Delays Model: expanding the three delays model with evidence from Madagascar for maternal referrals in LMICs. BMJ Glob Health. 2026;11(2). doi:10.1136/bmjgh-2025-020936
- Thaddeus S, Maine D. Too far to walk: Maternal mortality in context. Soc Sci Med. 1994;38(8):1091–110. doi:10.1016/0277-9536(94)90226-7
- Andersen BL, Cacioppo JT. Delay in seeking a cancer diagnosis: delay stages and psychophysiological comparison processes. Br J Soc Psychol. 1995;34(Pt 1):33–52. doi:10.1111/j.2044-8309.1995.tb01047.x
- Walter F, Webster A, Scott S, Emery J. The Andersen Model of Total Patient Delay: a systematic review of its application in cancer diagnosis. J Health Serv Res Policy. 2012;17(2):110–8. doi:10.1258/jhsrp.2011.010113
- Weller D, Vedsted P, Rubin G, et al. The Aarhus statement: improving design and reporting of studies on early cancer diagnosis. Br J Cancer. 2012;106(7):1262–7. doi:10.1038/bjc.2012.68